Figure 5
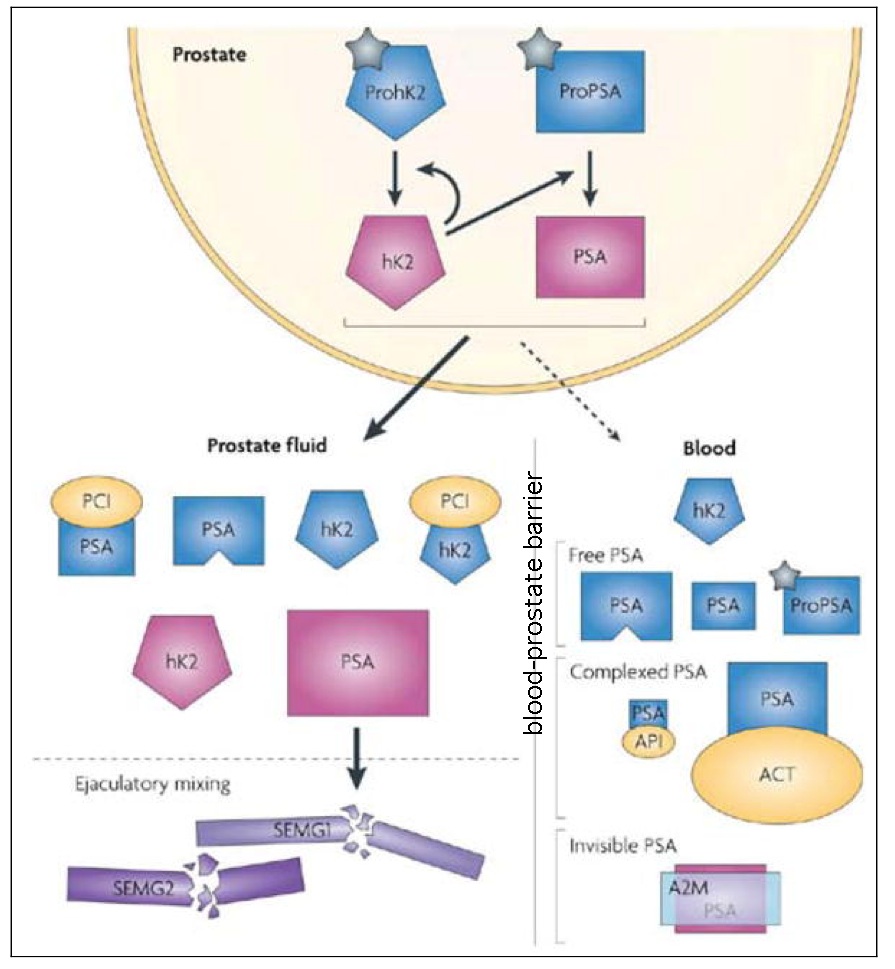
Prostate-specific antigen (PSA) subforms and interactions
Active forms of PSA and kallikrein-related peptidase 2 (hK2) are shown in red, inactive forms in blue or green. In the prostate, pro-peptides (grey wedge) are removed from proPSA and prohK2, leaving the mature, catalytic forms. hK2 might be one of the proteases responsible for these processing events. PSA and hK2 are released at high concentrations into prostatic fluid, then into seminal fluid, and at low concentrations into blood. PSA forms in prostatic fluid are active PSA, nicked PSA and PSA complexed with protein C inhibitor (PCI, encoded by SERPINA2), a protease inhibitor. The sizes in the figure indicate the relative abundances of the forms. In seminal fluid, active PSA is believed to be responsible for liquefaction of seminal fluid by proteolysing gel proteins (SEMG1 and SEMG2, which are secreted primarily by the seminal vesicles, though SEMG2 is also secreted in small amounts by the epididymis). Blood contains a variety of forms of PSA: free PSA forms (nicked, intact and proPSA) and complexed PSA. The most abundant form in blood is PSA complexed with α1-antichymotrypsin (ACT); complexes with α2-macroglobulin (A2M) or α1-protease inhibitor (API) are estimated to comprise only a 1–2% or lower proportion of PSA in blood. A2M envelopes PSA, masking the epitopes recognized by commercial PSA assays and thus rendering this form invisible to the assays. PSA levels in seminal fluid are 0.5–3.0 mg/ml (~106-fold higher than in blood) and hk2 levels in seminal fluid are 2–12 microg/ml (~104-fold higher than in blood).
(Reproduced, with permission, from Lilja, H. et al. Prostate-specific antigen and prostate cancer: prediction, detection and monitoring. Nature reviews cancer. 8, 268–278, 2008).48