|
|
Ältere
Bekanntmachungen
Neue Bekanntmachungen
(Datum: 4. Mai 2008)
Attorney General's Investigation Reveals Flawed Lyme Disease Guideline Process, IDSA Agrees To Reassess Guidelines, Install Independent Arbiter.
Blumenthal's findings include the following:
- The IDSA failed to conduct a conflicts of interest review for any of the panelists prior to their appointment to the 2006 Lyme disease guideline panel;
- Subsequent disclosures demonstrate that several of the 2006 Lyme disease panelists had conflicts of interest;
- The IDSA failed to follow its own procedures for appointing the 2006 panel chairman and members, enabling the chairman, who held a bias regarding the existence of chronic Lyme, to handpick a likeminded panel without scrutiny by or formal approval of the IDSA's oversight committee;
- The IDSA's 2000 and 2006 Lyme disease panels refused to accept or meaningfully consider information regarding the existence of chronic Lyme disease, once removing a panelist from the 2000 panel who dissented from the group's position on chronic Lyme disease to achieve "consensus"
- The IDSA blocked appointment of scientists and physicians with divergent views on chronic Lyme who sought to serve on the 2006 guidelines panel by informing them that the panel was fully staffed, even though it was later expanded;
- The IDSA portrayed another medical association's Lyme disease guidelines as corroborating its own when it knew that the two panels shared several authors, including the chairmen of both groups, and were working on guidelines at the same time. In allowing its panelists to serve on both groups at the same time, IDSA violated its own conflicts of interest policy.
IDSA has reached an agreement with Blumenthal's office calling for creation of a review panel to thoroughly scrutinize the 2006 Lyme disease guidelines and update or revise them if necessary. The panel -- comprised of individuals without conflicts of interest -- will comprehensively review medical and scientific evidence and hold a scientific hearing to provide a forum for additional evidence. It will then determine whether each recommendation in the 2006 Lyme disease guidelines is justified by the evidence or needs revision or updating.
(Datum: 25.4.2008)
Garth L. Nicolson, PhD (Department of Molecular Pathology, The Institute for Molecular Medicine, Huntington Beach, CA), Chronic Bacterial and Viral Infections in Neurodegenerative and Neurobehavioral Diseases, LABMEDICINE, Volume 39 Number 5, May 2008 (in cache)
Abstract:
Often, patients with neurodegenerative or neurobehavioral diseases have chronic, neuropathic infections that could be important in disease inception, disease progression, or increasing the types or severities of signs and symptoms. Although controversial, the majority of patients with various neurodegenerative or neurobehavioral conditions, such as amyotrophic lateral sclerosis, multiple sclerosis, Alzheimers disease, Parkinsons disease, and autistic spectrum disorders, show evidence of central nervous system or systemic bacterial and viral infections. For example, using serology or polymerase chain reaction evidence of Chlamydia pneumoniae, Borrelia burgdorferi, Mycoplasma species, human herpesvirus-1 and -6, and other bacterial and viral infections revealed high infection rates that were not found in control subjects. Although chronic infections were not found in some studies, and the specific role of chronic infections in neurological disease pathogenesis has not been determined or is inconclusive, the data suggest that chronic bacterial or viral infections could be common features of progressive neurodegenerative and neurobehavioral diseases.
(Datum: 1.4.2008)
Lyme-Induced Autism, East Coast 1-Day Conference, April 12, 2008. Free online Webcast Live from New Jersey
This 1-day conference will educate attendees with an Intermingling of Traditional and Alternative Therapies to provide treatment strategies to begin in our healing journey.
This conference will cover topics that would be appropriate for parents of children with autism, Lyme disease and related infections, adults with Lyme disease and medical professionals (You'll hear from Dr. Charles Ray Jones, Robert Bransfield, Richard Horowitz, Janelle Love, Guissepina Feingold, Warren Levin, Peta Cohen, Jeffrey Baker, and Ritchie Shoemaker)
(Datum: 26.3.2008)
Rupprecht TA, Koedel U, Fingerle V, Pfister HW, The Pathogenesis of Lyme Neuroborreliosis: From Infection to Inflammation, Mol Med. 2008 Mar-Apr; 14(3-4): 205-212.
This review describes the current knowledge of the pathogenesis of acute Lyme neuroborreliosis (LNB), from invasion to inflammation of the central nervous system.
Borrelia burgdorferi (B.b.) enters the host through a tick bite on the skin and may disseminate from there to secondary organs, including the central nervous system.
- To achieve this, B.b. first has to evade the host's immune system.
Borreliae possess several mechanisms that enable them to escape (Figure 1) including
-
downregulation of immunogenic surface proteins,
-
inactivation of effector mechanisms, or
-
hiding in less accessible compartments like the extracellular matrix.
 |
Figure 1 (im Cache)
Mechanisms of the borrelia to evade the immune system. Borrelia are recognized by immune cells through TLR2 and CD14 and attacked by complement and antibodies. Therefore, the borrelia downregulate their surface proteins, hide in the extracellular matrix, ( more ...)
|
- In a second step, the borrelia have to reach the central nervous system and cross the blood-brain barrier.
- Once in the cerebrospinal fluid (CSF), the spirochetes elicit an inflammatory response.

|
Figure 2 (im Cache)
The inflammatory B-cell response in the CSF in response to the CNS infection.
- Borrelia are recognized by monocytic cells
- which produce the B-cell–attracting chemokine CXCL13
- B cells immigrate into the CSF
and mature to plasma cells
( more ...)
|
We describe current knowledge about the infiltration of leukocytes into the CSF in LNB.
In the final section, we discuss the mechanisms by which the spirochetal infection leads to the observed neural dysfunction.

|
Figure 3 (im Cache)
The neural dysfunction in neuroborreliosis. Three principal mechanisms that lead to the injury of neuronal cells:
-
the secretion of cytotoxic substances by leucocytes and glial cells,
-
direct cytotoxicity, and
-
autoimmune-triggered processes
( more ...)
|
To conclude, we construct a stringent concept of the pathogenesis of LNB.

|
Figure 4 (im Cache)
Borrelia adhere to neuronal cells. Borrelia (arrows) are attached to cells of the neuronal cell line B50. The borrelia (B. garinii) were visualized using an OspA monoclonal antibody.
... spirochetal-induced, autoimmune-mediated mechanisms by “molecular mimicry” could also be an important step in the observed neural dysfunction. Cross-reactive antibodies can be found in Lyme borreliosis (104–106), as the serum of patients with Lyme disease contains antibodies against flagellin of B.b. that cross-react with neural antigens. In this context, it is of note that OspA is also supposed to play a role in autoimmune Lyme arthritis (30,107).
|
(Datum: 6.3.2008)
Über die Notwendigkeit, zusätzlich zu Ceftriaxon noch andere Antibiotika zu verwenden, um zystische, intrazelluläre und tief im Gewebe angesiedelte Borrelien zu erreichen (die Problematik der Nischen):
- Hodzic E, Feng S, Holden K, Freet KJ, Barthold SW. Persistence of Borrelia burgdorferi Following Antibiotic Treatment in Mice. Antimicrob Agents Chemother. 2008 Mar 3;
Results indicated that following antibiotic treatment, mice remained infected with non-dividing but infectious spirochetes, particularly when antibiotic treatment was commenced during the chronic stage of infection.
Lingering Bacteria Don't Indicate Chronic Lyme Disease, UC Davis News and Information, March 31, 2008
Media Contact: Stephen Barthold, Center for Comparative Medicine, +1 (530) 752-1245, swbarthold@ucdavis.edu
"This is just part of our world of microbes," Barthold said. "Antibiotics are designed to kill large numbers of bacteria -- to knock them down to the point that the body's immune system can get control of the infection."
"I suspect that if the initial round of antibiotics hasn't eliminated them, it's not likely that a longer regimen of antibiotics would be any more successful," Barthold said. "It's more likely that a completely different class of antibiotics would be needed to accomplish that. This laboratory mouse model will allow us to address those possibilities."
- Kersten A, Poitschek C, Rauch S, Aberer E
Effects of penicillin, ceftriaxone, and doxycycline on morphology of Borrelia burgdorferi. Antimicrob Agents Chemother 1995 May;39(5):1127-33
By transmission electron microscopy, intact spirochetal parts, mostly situated in cysts, were seen up to 96 h after exposure with all three antibiotics tested. According to experiences from studies with other spirochetes it is suggested that encysted borreliae, granules, and the remaining blebs might be responsible for the ongoing antigenic stimulus leading to complaints of chronic Lyme borreliosis.
- Mehr Literatur
Karen P. Yerger, Rita L. Stanley, Confronting Lyme Disease: What Patient Stories Teach Us
Lyme disease is the most prevalent tick-borne illness in the United States today with as many as a quarter million infections occurring each year. For those who receive prompt and adequate treatment, full recovery is achievable. However, for many individuals, delayed and inadequate treatment has resulted in chronic and debilitating illness.
(Datum: 4.3.2008)
Danke, Corry!
(Datum: 16.2.2008)
-
Jahresversammlung der Deutschen Borreliose-Gesellschaft
Freitag, 18. - Samstag 19. April 2008
Goslar-Hahnenklee
Programm
Eingeladene Vorträge
Therapiekonzepte der Borreliose im Wandel der Zeit
25 Jahre Erfahrung - Rückblick und Ausblick in Praxis und Forschung
Dr. med. Laurence Meer-Scherrer, Flamatt, Schweiz
Hautmanifestationen der Lyme-Borreliose
Akad. Dir. i.R. Dr. med. Uwe Neubert, FA für Dermatologie, Großhadern, München
Immunologie der Borrelien-Infektion
Prof. Dr. med. Rüdiger von Baehr, FA für Innere Medizin, IMD Berlin
Die Borreliose-Erkrankung und ihre neuro-psychiatrischen Symptome
Dr. med. Martina Lorenz, FÄ für Neurologie und Psychiatrie, Springe
Diagnose chronisch entzündlicher Prozesse im Bewegungsapparat, Nervensystem und Vegetativum als Hinweis auf eine borrelioseinduzierte Intoxikation
Prof. Dr. med. Werner Grossmann, FA für Pharmakologie und Neurologie, München
Dr. med. Christine Bachmann, FÄ für Orthopädie, München
Alzheimer's disease: The emerging role of infection
Dr. Judith Miklossy, M.D.
The University of British Columbia, Kinsmen Laboratory of Neurological Research, Vancouver, BC, Canada
Leitung und Organisation
Prof. Dr. med. Rüdiger von Baehr,
Institut für medizinische Diagnostik, Berlin
Prof. Dr. rer. nat. Hartmut Prautzsch,
Universität Karlsruhe
- Ogden NH et al. The role of migratory birds in introduction and range expansion of Ixodes scapularis ticks, and Borrelia burgdorferi and Anaplasma phagocytophilum in Canada. Appl Environ Microbiol. 2008 Feb 1 (related articles)
- The prevalence of birds carrying I. scapularis ticks (mostly nymphs) was 0.35% (95%
confidence interval [CI] = 0.30 - 0.42), but
- a nested study by experienced
observers suggested a more realistic infestation prevalence of 2.2% (95% CI =
1.18 -3.73).
- Mean infestation intensity was 1.66 per bird.
- Overall, 15.4% of I.
scapularis nymphs (95% CI = 10.7 - 20.9) were PCR-positive for Borrelia
burgdorferi, but only 8% (95% CI = 3.8 - 15.1) were positive when excluding
nymphs collected at Long Point, Ontario where B. burgdorferi is endemic.
(Datum: 14.2.2008)
Noreen Turyn, The Lyme Controversy, a 3-part video, ABC 13, WSET-TV, Lynchburg, Virginia, USA, 12. February 2008.
(Datum: 24.1.2008)
Goldhagen H, Rawlings J, Fighting Back: How B burgdorferi Persists, 14th International Scientific Conference on Lyme Disease & Other Tick-Borne Disorders, June 6, 2001
What accounts for borreliae's ability to evade or suppress an effective immune response? According to Charles Pavia, PhD,[1] of the New York College of Osteopathic Medicine, New York Institute of Technology, Old Westbury, New York, there are at least 6 potential explanations:
- antigenic variation (this is seen with the Borrelia species that cause tick-borne relapsing fever) or differential expression of antigens (especially the outer surface proteins; with B burgdorferi, only OspC is expressed during mammalian infection)
- production of an outer protective coat (eg, capsule, as seen with T pallidum)
- atypical forms (eg, cyst-like variants)
- incomplete immune response (eg, insufficient antibody , T-cell , or phagocytic response)
- deranged host immune response (eg, host-, tick-, or spirochete-derived immunosuppressive factors)
- other evasive factors (eg, motility)
Pavia C, Mechanisms of persistency of the Lyme disease spirochete. Program and abstracts of the 14th International Scientific Conference on Lyme Disease and Other Tick-Borne Disorders; April 21-23, 2001; Hartford, Connecticut.
(Datum: 24.1.2008)
An Appraisal of "Chronic Lyme Disease", Correspondence, N Engl J Med. 2008 Jan 24;358(4):428-431
Original article: Feder HM Jr, Johnson BJ, O'Connell S, Shapiro ED, Steere AC, Wormser GP; Ad Hoc International Lyme Disease Group, A critical appraisal of "chronic Lyme disease". N Engl J Med. 2007 Oct 4;357(14):1422-30
(Datum: 9.11.2007)
- Hajek T, Libiger J, Janovska D, Hajek P, Alda M, Hoschl C., Clinical and demographic characteristics of psychiatric patients seropositive for Borrelia burgdorferi, Eur Psychiatry. 2006 Mar;21(2):118-22
CONCLUSION: These findings elaborate on potential association between Bb infection and psychiatric morbidity, but fail to identify any specific clinical 'signature' of Bb infection.
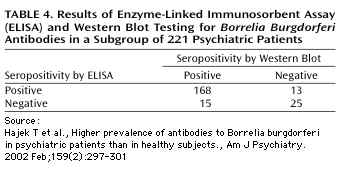
- Hajek T, Paskova B, Janovska D, Bahbouh R, Hajek P, Libiger J, Hoschl C. Higher prevalence of antibodies to Borrelia burgdorferi in psychiatric patients than in healthy subjects, Am J Psychiatry. 2002 Feb;159(2):297-301. (free full text)
CONCLUSIONS: These findings support the hypothesis that there is an association between Borrelia burgdorferi infection and psychiatric morbidity. In countries where this infection is endemic, a proportion of psychiatric inpatients may be suffering from neuropathogenic effects of Borrelia burgdorferi.
- Ein aufschlußreiches Ergebnis am Rande der Publikation #2
(Datum: 7.11.2007)
- Bransfield RC, Wulfman JS, Harvey WT, Usman AI. The association between tick-borne infections, Lyme borreliosis and autism spectrum disorders. Med Hypotheses. 2007 Nov 1; [Epub ahead of print]
PMID: 17980971
- Filme über Borreliose
- The Lyme Disease Controversy, Lyme Disease Research Studies, New York State Psychiatric Institute, Columbia University, New York.
(Datum: 21.10.2007)
B. A. Fallon MD*, J. G. Keilp PhD, K. M. Corbera MD, E. Petkova PhD, C. B. Britton MD, E. Dwyer MD, I. Slavov PhD, J. Cheng MD, PhD, J. Dobkin MD, D. R. Nelson PhD, and H. A Sackeim PhD
From the Department of Psychiatry (B.A.F., J.G.K., K.M.C., E.P., I.S., J.C., H.A.S.), Department of Biostatistics (E.P.), Department of Neurology (C.B.B.), Department of Medicine (E.D., J.D.), and New York State Psychiatric Institute (B.A.F., J.G.K., K.M.C., E.P., I.S., J.C., H.A.S.), Columbia University, New York; and Department of Cell and Molecular Biology, University of Rhode Island, Kingston (D.R.N.).
A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy, Published online before print October 10, 2007
(Neurology 2007, doi:10.1212/01.WNL.0000284604.61160.2d)
Background: Optimal treatment remains uncertain for patients with cognitive impairment that persists or returns after standard IV antibiotic therapy for Lyme disease.
Conclusion: IV ceftriaxone therapy results in short-term cognitive improvement for patients with posttreatment Lyme encephalopathy, but relapse in cognition occurs after the antibiotic is discontinued. Treatment strategies that result in sustained cognitive improvement are needed.
Anmerkung von J. Gruber:
Dies ist der in-vivo Nachweis eines von Klempner et al. in-vitro gefundenen Effekts: Wenn man extrazellulär wirkende Antibiotika zu früh absetzt, kehrt die extrazelluläre Krankheit zurück.
Sie hatten eine in-vitro Borrelienkultur mit Ceftriaxon abgetötet, und die Kultur blieb steril. Aber als sie Fibroblaste der Kultur hinzufügten und 14 Tage mit derselben Ceftriaxon-Konzentration abtöteten, war die Kultur nur anfänglich steril. Nach einiger Zeit erschienen wieder lebende, vermehrungsfähige Borrelien in der Kultur.
- Georgilis K, Peacocke M, Klempner MS, Fibroblasts protect the Lyme disease spirochete, Borrelia burgdorferi, from ceftriaxone in vitro. J Infect Dis. 1992 Aug;166(2):440-4.
- Klempner MS, Noring R, Rogers RA, Invasion of human skin fibroblasts by the Lyme disease spirochete, Borrelia burgdorferi. J Infect Dis. 1993 May;167(5):1074-81.
(Datum: 9.9.2007)
Ardith Bondi, Summary of Letters of Testimony
which were sent to Assemblyman Richard N. Gottfried, Chairman,
New York State Assembly Committee on Health,
for inclusion with the records of the hearing on
Long Term Antibiotic Treatment of Lyme Disease
(in cache) which took place at the New York State Assembly, November 27, 2001
(Datum: 6.9.2007)
Stellungnahme zur Verbesserung der Kenntnisse über das Infektions- und Erkrankungsrisiko der Lyme-Borreliose - Aufnahme in das Infektionsschutzgesetzt
Der Bundesverband Zeckenkrankheiten (BZK) hat in seiner letzten Mitgliederversammlung eine Stellungnahme zur Aufnahme der Lyme-Borreliose in das Infektionsschutzgesetz verabschiedet. die Stellungnahme ist inzwischen an die Mitglieder der Gesundheitsausschüsse von Bund und Land sowie dem RKI und weiteren Bundesinstituten versand worden. Entsprechende Gespräche laufen hier bereits.
Wünschenswert ist eine breite Unterstützung aller Organisationen, die sich mit der Lyme-Borreliose beschäftigen. Wir möchten Sie deshalb bitten auf diese Stellungnahme hinzuweisen und sie auf Ihrer Seite zu verlinken.
Die Printversion kann beim BZK angefordert werden - oder aber Sie drucken diese aus und geben Sie an interessierte Personen weiter (Wir weisen aber darauf hin, dass dazu die Originalversion verwendet werden muß.)
Des Weiteren wurde die Gesundheitspolitische Stellungnahme zur Lyme-Borreliose akutalisiert. Auch diese Version kann unter den o.a. Bedingungen ausgedruckt und an Interessierte weitergegeben werden.
Stellungnahmen des BZK
Jutta Zacharias
(Datum: 3.8.2007)
Yael Waknine, Rocephin Plus Calcium Linked to Fatal Reactions in Neonates, Medscape Alerts, July 6, 2007.
Oksi J, Nikoskelainen J, Hiekkanen H, Lauhio A, Peltomaa M, Pitkaranta A, Nyman D, Granlund H, Carlsson SA, Seppala I, Valtonen V, Viljanen M., Duration of antibiotic treatment in disseminated Lyme borreliosis: a double-blind, randomized, placebo-controlled, multicenter clinical study, Eur J Clin Microbiol Infect Dis. 2007 Aug;26(8):571-81.
"... The aim of this multicenter study was to determine whether initial treatment with intravenous ceftriaxone for 3 weeks should be extended with a period of adjunct oral antibiotic therapy. ..."
"... The results indicate that oral adjunct antibiotics are not justified in the treatment of patients with disseminated LB who initially receive intravenous ceftriaxone for 3 weeks. The clinical outcome cannot be evaluated at the completion of intravenous antibiotic treatment but rather 6-12 months afterwards. In patients with chronic post-treatment symptoms, persistent positive levels of antibodies do not seem to provide any useful information for further care of the patient. ..."
(Datum: 26.7.2007)
Dr. Gregory Bach, Do.O., P.C. 2415 North Broad Street, Colmar, PA 18915, USA "Recovery of Lyme Spirochetes by PCR in Semen Samples of Previously Diagnosed Lyme Disease Patients, International Scientific Conference on Lyme Disease, April, 2001.
"... Our laboratory studies confirm the existence of Lyme spirochetes in semen/vaginal secretions. ... "
Schmidt BL, Aberer E, Stockenhuber C, Klade H, Breier F, Luger A, "Detection of Borrelia burgdorferi DNA by polymerase chain reaction in the urine and breast milk of patients with Lyme borreliosis." Diagn Microbiol Infect Dis. 1995 Mar;21(3):121-8.
" ... In addition to urine, breast milk from two lactating women with erythema migrans was tested and also found reactive. Borrelia burgdorferi DNA can be detected with high sensitivity (91%) by a nested PCR in urine of patients with Lyme borreliosis. ..."
(Datum: 16.5.2007)
The 6th UK Tick Borne Conference will be on Friday 6th July 2007, at Stamford Hall, Leicester University, Stoughton Drive South, LE2 2ND. This year our main speaker will be Dr Joseph Burrascano, author of "Diagnostic Hints and Treatment Guidelines for Lyme and Other Tick Borne Illnesses".
Other speakers also confirmed:
Dr David Owen, Professor Terry J Daymond, Dr Sarah Chissel, Dr Victoria Cairns, Dr Marie Kroun, Dr Andy Wright
(Datum: 22.3.2007)
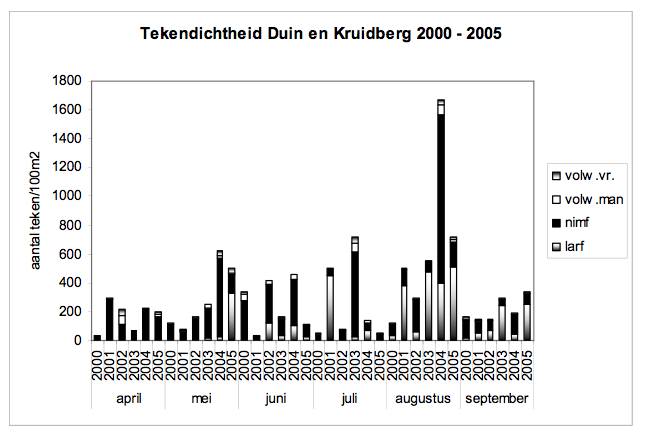
Zeckendichte in Dünen in Kruidberg (Niederlande), aufgeteilt nach Entwicklungsstadien
Quelle: Fred Borgsteede, Cor Gaasenbeek, Albert de Boer, Jeroen Dijkstra (Animal Sciences Group WUR, Divisie Infectieziekten, Postbus 65, 8200 AB Lelystad ) et al. Het verloop van tekenpopulaties en de besmetting van teken met Borrelia en Ehrlichia: Resultaten van onderzoek in de periode 2000-2005, Wageningen UR, 2006. (im Cache). Danke, Corry, für den Hinweis!
(Datum: 22.2.2007)
Megan M. Blewett, A Geostatistical Analysis of Possible Spirochetal Involvement in Multiple Sclerosis and Other Related Diseases, Canadian Lyme Diseaase Foundation, 22 February 2007. (im Cache)
... Producing the maps and data required contacting all of the state epidemiologists in the nation for Lyme incidence data. Compiling the data has resulted in one of the most comprehensive Lyme databases available to researchers. The results of the visual, geostatistical, and biochemical analyses suggest common spirochetal involvement in MS and related diseases.
(Datum: 4.12.2006)
Maraspin V, Lotric-Furlan S, Strle F., Development of erythema migrans in spite of treatment with antibiotics, Wien Klin Wochenschr. 2002 Jul 31;114(13-14):616-9.
RESULTS: Seven of 5056 (0.14%) patients,
diagnosed with typical erythema migrans, developed the skin lesion despite receiving antibiotics after a tick bite.
(Datum: 27.10.2006)
ILADS Demands Retraction of New IDSA Guidelines for Treatment of Lyme Disease, US Newswire, 27 Oct. 2006
... In a point-by-point analysis of the guidelines,
(in cache:
Dr. [Raphael] Stricker states [Infectious Diseases Society's] IDSA's position reflects a biased view of the disease that's either unsubstantiated or refuted by existing peer- reviewed medical literature. "The IDSA's 'one-size fits all' approach to Lyme diagnosis and treatment will result in misdiagnosis and denial of care to thousands of patients annually," writes Dr. Stricker in the letter to Dr. Gorbach "creating a public health burden as...patients become chronically ill and disabled." ...
[Dr. Sherwood Gorbach is editor of 'Clinical Infectious Diseases' that published the paper
Wormser GP, et al. "The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America, Clin Infect Dis. 2006 Nov 1;43(9):1089-134. Epub 2006 Oct 2]
Petition
Wir, die Unterzeichner, sind schwer beunruhigt durch die neuen Borreliose-Richtlinien der Infectious Disease Society of America (IDSA). Diese Richtlinien verlangen für die Diagnose von Borreliose absolutes Verlassen auf
- entweder das Vorweisen eines Erythema migrans (ECM)
- oder positive serologische Bluttests
und empfehlen streng begrenzte antibiotische Therapie-Verläufe, wenn entweder eine Wanderröte oder ein positiver Test vorliegen ....
Hier kann man die Petition unterschreiben.
(Datum: 19.7.2006)
Zertifizierte Arztfortbildung zur Diagnose und Therapie der Lyme-Borreliose, Aggertalklinik, 30. September 2006.
Vorträge und Diskussionsleitung:
- Prof. Dr. med. Rüdiger von Baehr (Interne Medizin und Immunologie),
- Prof. Dr. med. Ernst Fink (Biologie, Zoologie)
- Prof. Dr. med. Hans-Jürgen Hütter (Laboratoriumsmedizin)
- Dr. med. Wolfgang Klemann (Interne Medizin)
- Prof. Dr. rer. nat. Hartmut Prautzsch (Vorsitz, Borreliose-Gesellschaft, Betriebs- und Dialogsysteme, Angewandte Geometrie und Computergraphik)
- Cord Uebermuth (Augenheilkunde)
- Dr. med. Jochen Viebahn (Allgemeine Medizin)
(Datum: 13.7.2006)
Klempner-Studie
Klempner et al. demonstrierten, daß ein unzureichendes antibiotisches Regime bei der Behandlung von chronischer Borreliose nicht besser war als ein Placebo [Klempner MS, Hu LT, Evans J, Schmid CH, Johnson GM, Trevino RP, Norton D, Levy L, Wall D, McCall J, Kosinski M, Weinstein A., Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001 Jul 12;345(2):85-92.]
Kritik an der "Klempner-Studie"
-
Review by independent consulting company
- Phillips S, Bransfield R, Sherr V, Brand S, Smith H, Dickson K, and Stricker R:
Evaluation of Antibiotic Treatment in Patients with Persistent Symptoms of
Lyme Disease, An ILADS Position Paper, April, 2003
- Wikipedia review
- Analytic Perspective by Cameron DJ. Epidemiologic review of the generalizability of two clinical trials of Lyme disease conducted by Klempner et al., Epidemiologic Perspectives & Innovations, 2006
(Datum: 21.8.2006)
Phyllis Mervine, EdM, California Lyme Disease Association and Ron D. Keith, Marin/Sonoma Mosquito and Vector Control District,
Review: Risk of Infection From Tick Bite vs. Duration of Attachment of Ixodes Nymphs.
A poster along with much other information is available at the California Lyme Disease Association website. People should sign in as a Guest (no password is required). Posters are filed under Public Education Materials / Posters.
(Datum: 18.8.2006)
Infektion als Funktion der Dauer der Zeckenanhaftung
Sood SK, Salzman MB, Johnson BJ, Happ CM, Feig K, Carmody L, Rubin LG, Hilton E, Piesman J., Duration of tick attachment as a predictor of the risk of Lyme disease in an area in which Lyme disease is endemic.
J Infect Dis. 1997 Apr;175(4):996-9. PMID: 9086168 [PubMed - indexed for MEDLINE]
Piesman J, Mather TN, Sinsky RJ, Spielman A., Duration of tick attachment and Borrelia burgdorferi transmission. J Clin Microbiol. 1987 Mar;25(3):557-8.
(Datum: 17.8.2006)
Tick-Twister
O'TOM: "The easiest and safest way to remove ticks, quickly, without leaving the mouthparts in the skin, without any chemicals."
|
 |
 |
| Choose the most suitable hook,
according to the size of the tick
|
Engage the hook by approaching
the tick from the side (the body
of a tick is flat) until it is held
|
Lift the hook very lightly and
TURN IT (screwing or unscrewing) |
The tick detaches by itself after 2 or 3 rotations.
Video Show
Wo man das kaufen kann
Vertrieb für Deutschland:
Fett sales & marketing,
Postfach 1404,
56404 Montabaur.
Kontakt:
Katja Remy,
phone: 00 49 (0) 2602 - 999 56 56
fax: 00 49 (0) 2602 - 999 56 58
Preis für ein Paar, d.h. einen großen und einen kleinen Haken: 1.99 EUR, Mindestabnahme: 48 Paare
Verkauf eines Paares (Preis: 2 EUR zzgl. Portokosten)
(Datum: 12.5.2006)
Liebe Freunde und Mitstreiter der Borreliose-Selbsthilfe,
am 17. Juni findet in Dippoldiswalde unser erstes Symposium zur Borreliose statt (eine ausführliche Einladung mit Veranstaltungsort und Programm).
Für alle, die nicht wissen wo Dippoldiswalde liegt:
Dippoldiswalde liegt ca. 25 Km südlich von Dresden an der B170 Dresden-Prag im Osterzgebirge. Die Fahrzeit von und nach Dresden beträgt ca. 25 Minuten. Wenn Sie unsere Veranstaltung für einen Kurzurlaub nutzen wollen, senden ich Ihnen gerne ein Übernachtungsverzeichnis zu.
Ich würde mich freuen, Sie am 17. Juni hier in Dippoldiswalde begrüßen zu können.
Mit freundlichen Grüßen
Jens Wriedt
Leiter der Borreliose-SHG Dippoldiswalde
(Datum: 13.4.2006)
Isabel Diterich, Immunomodulation and new therapeutic strategies in Lyme borreliosis, Dissertation (Dr. rer. nat.), Universität Konstanz, 2003.(im Cache)
7 Summary
If infection with Borrelia burgdorferi is not treated adequately with antibiotics in an early stage, it may lead to Lyme borreliosis (LB), a chronic multisystemic disorder which is difficult to cure. In some cases the pathogen survives in spite of antibiotic treatments. It is challenging to understand why Borrelia are often not eradicated, although being recognized by the host's immune defense and occasionally inducing a strong inflammatory reaction. Thus, it remains an area of debate how this pathogen
persists in human tissues.
This question was addressed in the present thesis, examining possible immune evasion mechanisms of Borrelia.
- Blood cells from patients suffering from persistent LB released significantly lower levels of pro-inflammatory cytokines (TNFa and IFNg) in response to either Borrelia lysate or to lipopolysaccharide (LPS) in comparison to cells from healthy volunteers.
- In blood from healthy volunteers Borrelia lysate led to strong production of anti-inflammatory IL-10 and G-CSF, while inducing only low levels of proinflammatory IFNg, compared to LPS.
- Similar to endotoxin tolerance, different Borrelia preparations desensitized human blood monocytes on re-stimulation with either stimulus.
- Borrelia-specific stimuli induced cross-tolerance towards heterelogous stimuli such as lipopolysaccharid (LPS) and lipoteichoic acid (LTA) in human monocytes.
- Toll-like receptor (TLR) 2 but not TLR4 was required for Borrelia-induced tolerance and cross-tolerance, as shown in experiments with knock-out mice.
- PBMC tolerized by Borrelia lysate exhibited reduced TLR2-mRNA levels.
Further, IL-10 was identified as a key mediator involved in tolerance-induction by Borrelia lysate.
- Combination of Filgrastim treatment with Ceftriaxone in a late stage LB-patient who failed standard antibiotic therapy led to successful eradication of the pathogen and complete regression of symptoms.
- The mouse model of Borrelia infection was set up and characterized in order to study the therapeutic effects of Filgrastim in vivo.
- Treating immunocompetent and immunodeficient SCID mice with Filgrastim, as an immunosupportive therapy of LB did not attenuate the characteristic ankle swelling induced by Borrelia infection.
- Regular application of Filgrastim led to an enhanced elimination of Borrelia from various organs in SCID mice. In immunocompetent mice this effect was less pronounced.
In summary, we propose that Borrelia modulate the host's immune system in order to evade clearance in the immunologically competent host. Tolerance could represent the mechanism inhibiting host response thereby enabling survival and persistence of the pathogen. Promising results were obtained testing a novel treatment strategy for late stage LB, a combination of Filgrastim as an immunosupportive therapy with antibiotics. The respective clinical trial based on these findings was recently started.
(Datum: 20.2.2006)
Arthur Weinstein (im Cache), Direktor des Diagnostic Immunology Laboratory und ehemaliges Mitglied des Kommittees, das den heute angewandten Standard für Lyme-Tests ("Dearborn criteria", Two-Tiered Testing") entwickelte, sagte,
daß Western Blots unter anderem deshalb nicht gleich sondern erst zur Bewertung eines ELISA angewendet werden, weil sie zu arbeitsintensiv und teuer seien, im Gegensatz zu ELISA, der ein automatisierter Test sei:
"Was unzuverlässig ist, ist die Interpretation der Resultate durch Ärzte unf Patienten" (A. Weinstein).
Die Kosten der Reagenzien für einen Westernblot liegen bei etwa 15 Euro.
(Datum: 7.2.2006)
Hunfeld KP, Ruzic-Sabljic E, Norris DE, Kraiczy P, Strle F, In Vitro Susceptibility Testing of Borrelia burgdorferi Sensu Lato Isolates Cultured from Patients with Erythema Migrans before and after Antimicrobial Chemotherapy, Antimicrob Agents Chemother. 2005 Apr;49(4):1294-301.
Our study substantiates borrelial persistence in some EM patients at the site of the infectious lesion despite antibiotic treatment over a reasonable time period.
In summary, our study provides compelling evidence that, although rare, survival of B. burgdorferi sensu lato can occur in antibiotically treated individuals with EM after antimicrobial chemotherapy. Spirochete persistence in these patients was not caused by increasing Minimum Inhibitory Concentrations or Minimal Bactericidal Concentrations for B. burgdorferi sensu lato. Instead, our findings corroborate those of Hansen et al. and Pfister et al. in relapsed patients with early LB, demonstrating that isolates cultured after the conclusion of roxithromycin and ceftriaxone therapy remain fully susceptible to these agents in vitro. These findings, however, do not rule out phenotypic resistance mechanisms similar to those assumed to cause relapse in syphilis and leptospirosis.
References
Hansen, K., A. Hovmark, A. M. Lebech, K. Lebech, I. Olsson, L. Halkier-Sorensen, L., E. Olsson, and E. Asbrink. 1992. Roxithromycin in Lyme borreliosis: discrepant results of an in vitro and in vivo animal susceptibility study and a clinical trial in patients with erythema migrans. Acta Dermato-Venereol. 72:297-300
Pfister, H. W., V. Preac-Mursic, B. Wilske, E. Schielke, F. Sorgel, and K. M. Einhaupl. 1991. Randomized comparison of ceftriaxone and cefotaxime in Lyme neuroborreliosis. J. Infect. Dis. 163:311-318.
Panconesi, E., G. Zuccati, and A. Cantini. 1981. Treatment of syphilis: a short critical review. Sex. Transm. Dis. 8:321-325, 37,
Straubinger, R. K., B. A. Summers, Y. F. Chang, and M. J. G. Appel. 1997. Persistence of Borrelia burgdorferi in experimentally infected dogs after antibiotic treatment. J. Clin. Microbiol. 35:111-116
(Datum: 29. 12. 2005)
SOME BACKGROUND INFORMATION:
Most of you know Monica Miller the lobbyist that has
worked with us in NYS for the past five years to help
protect our doctors from harassment by the state
medical disciplinary board, the OPMC.
Although Monica certainly gave her heart and soul to
helping us, her employer was actually the Foundation
for the Advancement of Innovative Medicine (FAIM).
That organization was made up of alternative
physicians who had also been targeted by the OPMC.
I want to thank all of you who contributed to FAIM so
they could continue to employ Monica to the point of
winning a victory with the OPMC.
When we started out fighting in NYS, most legislators, frankly, thought we were nuts. Monica taught us
how to talk with them and how to build support and
strategy as a grass roots organization. She herself
lobbied tirelessly, bringing some of the most
difficult legislators on board.
The combination of Monica, the LDA, the grassroots
groups, and those three wonderful champions of Lyme
disease in the state assembly (Mayersohn, Bradley, and
Miller), led us to a victory this year in the form of
the memo from the OPMC director protecting Lyme docs
from being targeted for their medical views.
The next step in New York will be to finally pass the
OPMC legislation so that the protection is nailed down
in law and we do not have to renegotiate with every
OPMC official in the future.
THE NEWS:
I'll give the bad news first, then follow with the
real good news.
- The BAD news for us is that FAIM has been unable to
continue employing Monica. She will no longer be a
lobbyist.
- The good news for us is that Monica will now be
working for the head of the Assembly health committee, Richard Gottfried. As you may know, Gottfried has
been a strong defender of Lyme disease patients.
Having Monica, with her understanding of and
commitment to Lyme issues ,on the inside of the state
government should be good enough news to compensate
for losing her help as a lobbyist.
Ellen
------ ANNOUNCEMENT FROM MONICA MILLER -------
I am joining the staff of New York Assemblyman
Richard Gottfried, Chairman of the Health Committee,
where I will work on a range of health care
legislation in that committee. As you may recall, Mr.
Gottfried was our primary sponsor for both medical
necessity and OPMC reform. I am delighted to be able
to continue supporting freedom of treatment choice in
this new capacity.
My website Healthlobby.com will close on December 31
along with related email addresses. Old phone numbers
and mailing address will become private.0ä3 If you wish
to contact me on legislative business please use the
legislative office number, 518-455-4941.
May I please extend my best wishes to you
in this season of light renewing.
(Datum: 9. 12. 2005)
Jutta Zacharias und der neue Dachverband der Selbsthilfe im Bereich Zecken-Krankheiten
Am 30.10.2005 wurde ein neuer Dachverband der Selbsthilfe im Bereich Zecken-Krankheiten (BZK) gegründet. Die Informationen auf meiner bisherigen Homepage werden neben vielen anderen weiteren interessanten Infos auf der neuen Seite des BZK zu finden sein. Einige meiner Artikel sowie die Interviews wurden deshalb in ein pdf-Format geändert. Sie stehen aber inhaltlich unverändert auf der Seite des BZK zur Verfügung.
Auch die Domain werde ich dem BZK überlassen. Dessen Seite wird zukünftig auch noch unter zwei weiteren Domains zu finden sein. Dies wird als Hauptdomain www.bzk-online.de mit Umleitungen www.bundesverband-zeckenkrankheiten und www.borreliose.org sein. Die Umleitungen werden Anfang nächsten Jahres vorgenommen.
Aktuell können Sie die Infos des BZK jetzt auf www.borreliose.org aufrufen.
Ich hoffe sehr, dass Sie die Arbeit des BZK mit Rat und Tat unterstützen werden.
Mit freundlichen Grüßen
Jutta Zacharias
Wir bewundern Dich, Jutta.
Jochen und Marianne
(Datum: 19. 11. 2005)
-
Stricker RB1, Lautin A2, Burrascano JJ3, Lyme disease: point/counterpoint, Expert Review of Anti-infective Therapy
April 2005, Vol. 3, No. 2, Pages 155-165 (im Cache)
1
Raphael B Stricker,
California Pacific Medical Center,
450 Sutter Street, Suite 1504, San Francisco, CA 94108,
USA, Tel.: +1 415 399 1035, Fax: +1 415 399 1057,
rstricker@usmamed.com,
2Andrew Lautin,
New York University School of Medicine, New York, NY, USA,
3Joseph J Burrascano,
East End Medical Associates, East Hampton, NY, USA
Two major clinical hurdles are
- the absence of a therapeutic end point in treating Borrelia burgdorferi and
- the presence of tickborne coinfections
... the affinity of Borrelia burgdorferi for multiple cell types and the presence of nonreplicating forms of the Lyme disease spirochete have contributed to persistent infection and failure of simple antibiotic regimens...
The spirochaete can enter cells such as fibroblasts, synovial cells, endothelial cells, and macrophages. In these cells, it becomes functionally resistant to treatment,
- partly due to "camouflage" proteins produced by itself or adsorbed from the cell, and
- partly due to altered morphology as the spirochaete assumes a non-replicating cyst form...
The optimal antibiotic regimen for chronic Lyme disease remains to be determined.
- Cluss RG, Silverman DA, Stafford TR, Extracellular secretion of the Borrelia burgdorferi Oms28 porin and Bgp, a glycosaminoglycan binding protein, Infect Immun. 2004 Nov;72(11):6279-86.
In the mammalian milieu, B burgdorferi uses the host fibrinolytic system to penetrate the blood-brain barrier and gain access to the central nervous system. The Lyme disease spirochaete contains a secretory mechanism for porin, adhesin, and haemolysin proteins, and these secreted products can contribute to the invasive properties of the organism.
- Steven E Phillips, Nick S Harris, Richard Horowitz, Lorraine Johnson and Raphael B Stricker, Lyme disease: scratching the surface, The Lancet 2005; 366:1771, DOI:10.1016/S0140-6736(05)67721-5
(Datum: 8. 10. 2005)
The Greater Hartford Lyme Association website
offers videos of some contributions to the conference the Association
held in Hartford in the spring of 2005. You
can order the DVD of the conference on the website.
Speakers:
(Datum: 6. 10. 2005)
Nach drei Jahren hat Joe Burrascano wieder eine neue Version (die 15. Ausgabe, September 2005) seiner Richtlinien publiziert.
(Datum: 20.9.2005)
Das 5. Kasseler Borreliose - Symposion findet am 29. Oktober 2005 im Bürgerhaus Obervellmar statt.
(Datum: 22.8.2005)
Trevor G. Marshall (Autoimmunity Research Foundation), How Borrelia evades the immune system, and how we help the immune system kill this Th1 bacterium, 30th Anniversary of Lyme Disease, Greater Hartford Lyme Group, Farmington, CT, May 7, 2005 (Dauer: 46 Minuten). Die DVD dieses Vortrags zeigt die Dias besser als das Internet. Man kann sie bei Trevor Marshall bestellen.
Dr. Marshall spends some time explaining how the antibiotics work best, explaining how bacteriostatic antibiotics could be chosen which symbiotically act on both the 30S and 50S subunits of the bacterial 70S Ribosome, making it very difficult for the bacteria to manufacture the proteins they need to survive. He explains why the Beta-Lactams are purely
palliative. He argues why there is no
possibility of killing the intra-phagocytic bacteria (which cause the
chronic Th1 diseases) without significant destruction of white cells,
without significant cytokine release, without significant sickness.
(Datum: 12.8.2005)
Prof. Dr. Fritz Schardt
früher: Betriebsärztliche Untersuchungsstelle, Bayerische Julius-Maximilians-Universität, Würzburg. Fritz.Schardt@mail.uni-wuerzburg.de,
jetzt (Stand März 2009): Predia - Gesellschaft für Prävention und Diagnostik mbH, Virchowstr. 22, 97072 Würzburg, Tel.: +49 931 - 80 49 60, Montag und Donnerstag 9 - 17 Uhr. Er hat keine Kassenzulassung. Kassenpatienten zahlen in der Regel eine Beratungsgebühr von 40 bis 60 Euro inkl. Rezept.)
- A New Approach to Chronic Lyme Disease (im Cache)
... Diflucan behindert ein Enzym mit Namen Cytochrom P450. Dies ist ein Enzym, das z.B. unsere Leber benutzt, um Chemikalien und Medikamente in ungiftige Formen zu überführen. Borrelia hat eine sehr primitive P450-Abwehr, sodaß -wenn man es behindert-, es leicht geschwächt wird. Daher glaube ich, daß Diflucan das Wachstum und die Vermehrung von Borrelien behindert. Es bringt sie nicht notwendigerweise um. Zusätzlich dringt es gut in Zellen ein und ins Nervensystem und das Gehirn, wo die Borrelien sich verstecken könnten...
... Diflucan war damals [als ich es zuerst benutzte] ein neues Medikament, das hauptsächlich gegen opportunistische Pilzinfektionen bei AIDS-Patienten eingesetzt wurde...
- Clinical effects of fluconazole in patients with neuroborreliosis, Eur J Med Res. 2004 Jul 30;9(7):334-6.
(Datum: 8.8.2005)
Nun ist es endlich soweit! Von unserer Veranstaltung am 5. 6. 2005 mit Frau Dr. Meer-Scherrer haben wir eine
DVD anfertigen lassen. Der Unkostenbeitrag beträgt einschließlich Versand 12,- EURO.
Bestellungen werden über Email oder Fax entgegen genommen.
Weitere Informationen über http://www.borreliose-berlin.de/index.html, auf Link "Veranstaltungen" clicken.
Hanna Priedemuth
(Datum: 6.8.2005)
Lyme Disease Medical Literature Summaries (Lyme Disease Symptoms, Persistence, Cysts, Seronegativity, Spirochetes)
(Datum: 10.7.2005)
Defizite in der "Leitlinie Neurologie: Neuroborreliose" der deutschen Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF)
Mir scheint, die Leitlinie Neurologie der Deutschen Gesellschaft für Neurologie gibt irreführende oder unklare Auskünfte zur intrathekalen Antikörper-Synthese, PCR an Liquorproben und zur Therapiedauer:
-
intrathekale Antikörpersynthese
- AWMF: "In 80 - 90 % der Neuroborreliosefälle kann die klinische Verdachtsdiagnose durch den Nachweis einer borrelienspezifischen intrathekalen Antikörpersynthese bestätigt werden."
- Patricia K. Coyle und Kollegen der State University von New York in der Stony Brook School of Medicine: "7% hatten intrathekale Antikörperproduktion, ein üblicher Test für Zentralllnervensystem-Infektion" (eine hinreichende aber nicht notwendige Bedingung für Neuroborreliose, siehe auch Neuroborreliose oder MS:
Entzündung durch Infektion oder Autoimmunprozeß?)
-
PCR (Polymerase Kettenreaktion)
- AWMF: "In den übrigen Fällen kann eine Borrelieninfektion durch den Nachweis borrelienspezifischer Nukleinsäuren mittels PCR im Liquor gestützt werden."
- Bettina Wilske: PCR hat im Liquor eine "Erfolgsrate" von ca. 10 - 20 %.
- Patricia K. Coyle: Positive [PCR-]Ergebnisse findet man in weniger als 40% [der Neuroborreliosefälle].
Hier sind Details.
-
Therapiedauer
- AWMF:"Bei der akuten Neuroborreliose wird meist eine Therapiedauer von 2 Wochen, bei der chronischen Neuroborreliose von 3 Wochen empfohlen. Allerdings gibt es keine Studie, die zeigt, daß bei der Neuroborreliose eine Therapiedauer von mehr als 2 Wochen bessere Ergebnisse bringt."
-
Krankheiten werden abhängig von ihrem Verlauf bei der Therapie behandelt. Daher erscheint mir die Angabe einer zeitlichen Begrenzung irrelevant. Der Kern von Lymenet.de ist eine Reihe von Papieren zur verlaufsabhängigen Therapie. Sie begleitete meine Diskussion mit Wissenschaftlern aus verschiedenen Fachgebieten.
Positiv formuliert: Die "Leitlinie Neurologie: Neuroborreliose" läßt Raum für den Fortgang der noch nicht abgeschlossenen Forschung auf diesem Gebiet. Formulierungen wie "kann .... bestätigt, gestützt werden, in den übrigen Fällen, wird meist empfohlen" und den Haftungsausschluß am Ende verstehe ich als einen Aufruf an uns, Eigenverantwortung für unsere Therapie zu übernehmen.
Zusätzliche Information:
Borrelien können innerhalb des Zentralnervensystems andere Antigene zeigen als außerhalb, und unsere Immunantwort darauf kann sich kontinuierlich verändern. Sie ist also nicht einfach digital, also vorhanden oder nicht vorhanden. Das muß bei der Interpretation des Liquor/Serum-Verhältnisses berücksichtigt werden.
Jochen Gruber
(Datum 20.5.2005)
Bacterium manipulates the human defence system:
The Borrelia bacterium is a master of disguise (im Cache)
20 May 2005
http://www.aka.fi/index.asp?id=78fc92314f6a4ed0b1dd1a690165a6ce
Borrelia bacteria are capable of masking themselves in the human body and deceiving the immune defence system. In this way they can hide in the human organism even for periods of years. In their recent studies Professor Seppo Meri and his team have managed to trace the evasive movements of the Borrelia bacterium in the body. Their work is part of the Microbes and Man research programme, jointly funded by the Academy of Finland and the Swedish Foundation for Strategic Research.
When they first enter the human organism, Borrelia bacteria do not always cause very intense inflammation. However, they proliferate unnoticed and later on the symptoms get worse. The immune system is unable in this situation to respond because the bacterium actively prevents any defensive reactions.
Professor Meri and his team have found that Borrelia bacteria, which are carried by ticks and birds, are capable of absorbing the protein that controls human inflammation (complement factor H). Normally, antibodies and the complement would kill off the bacteria, but this ingenious kidnap operation allows the Borrelia bacteria to disguise themselves and avoid being killed or devoured by inflammation cells. Consequently, the bacteria can continue to proliferate in the body and even reach the brain. An advanced bacterium may lead to a serious condition known as neuroborreliosis, which among other things may cause chronic headache or facial nerve paralysis.
One of the difficulties in diagnosing the symptoms caused by the Borrelia bacterium is that only half of all people who get a tick bite develop the tell-tale rash. Therefore, the bacterium often gets to make its way into the body and eventually into the bloodstream through the skin. Some one in ten patients are unable to shake off their symptoms even if they receive proper antibiotic treatment.
MICMAN is a three-year research programme in 2003-2005. The programme is a joint Finnish-Swedish venture funded by the Academy of Finland and the Swedish Strategic Research.
For further information:
Academy of Finland Communications
Tiina Pohjois-Koivisto,
tel. + 358 9 7748 8327, +358 40 833 2978, tiina.pohjois-koivisto@aka.fi
(Datum 12.5. 2005)
5. Kasseler Symposion, Bürgerhaus Obervellmar (bei Kassel), 29. Oktober, 2005, Anfang 14.00 Uhr.
Referenten sind Prof. Dr. Zipfel (HKI Jena), und Dr. Hunfeld, Frankfurt.
Anbei etwas, das mir so einfiel bez. Prof. Zipfel, und teils auch in den
Kasseler Berichten jetzt erwähnt wurde. Weiteres bitte via www.hki-jena.de,
Abt. Infektionsbiologie oder via IDW - Informationsdienst Wissenschaft.
Die Publikation von 29.7.02 ergab schon:
"....Diejenigen Borrelien, die dem Angriff des Immunsystems entgehen, sind in der Lage, bestimmte Eiweiße auf ihrer Oberfläche zu binden. Diese
Eiweiße, s.g. Komplementregulatoren, setzt der menschliche Körper
normalerweise ein, um seine eigene Zellen vor einer Zerstörung durch das Immunsystem zu schützen......"
Prof. Zipfel ist auch lehrend tätig für
Infektionsbiologie an der Uni Jena. Er ist seit 2000 Leiter der betr.
Abteilung beim HKI.
Auch bez. molekularer Mimikry anderer Erkrankungen erschien 7/2002 sein Artikel "Das tägliche Versteckspiel" (P.F. Zipfel, P. Kraiczy, J. Hellwage), in der auch die Borreliose erwähnt wird, in Biologie in unserer Zeit, 32, g. 2002, Nr. 6, 371-379.
Literatur:
- Cordes FS, Roversi P, Kraiczy P, Simon MM, Brade V, Jahraus O, Wallis R, Skerka C, Zipfel PF, Wallich R, Lea SM., A novel fold for the factor H-binding protein BbCRASP-1 of Borrelia burgdorferi, Nat Struct Mol Biol. 2005 Mar;12(3):276-7. Epub 2005 Feb 13.
- Kraiczy P, Hellwage J, Skerka C, Becker H, Kirschfink M, Simon MM, Brade V, Zipfel PF, Wallich R. Complement resistance of Borrelia burgdorferi correlates with the expression of BbCRASP-1, a novel linear plasmid-encoded surface protein that interacts with human factor H and FHL-1 and is unrelated to Erp proteins, J Biol Chem. 2004 Jan 23;279(4):2421-9. Epub 2003 Nov 7.
Dr. Hunfeld hat einiges publiziert bez. der Wirkung von Antibiotika auf Bb, war diesbez. auch in USA. Er hat auch auf Potsdamer "Zecken"-Symposien (z.B. 2001) referiert.
Corry Welker
(Datum: 31.3.2005)
Bundesweite Umfrage zur Behandlungssituation von an Borreliose Erkrankten und deren sozialen und ökonomischen Folgen für den Betroffenen und die Gesellschaft
Initiator der Umfrage: Jens Wriedt
Borreliose Selbsthilfegruppe Weißeritzkreis - Dippoldiswalde
Email: dippoldiswalde@borreliose-sachsen.de.
Die Aktion (begonnen im September 2004) wurde am 31.März 2005 beendet. Die Auswertung erfolgt je nach Stand Stück für Sück dann auf den gleichen Seiten.
Datum: 18.3.2005
- Die Prädilektionsstellen der bei einer Borrelien-Infektion möglichen Lymphadenosis cutis sind Ohrläppchen, Nase, Stirn und Mamillen. Bei einer geschwollenen Zehe denkt erst mal niemand an eine Borreliose, Praxis-Depesche 18/2004, S.10.
- Wahle M, Baerwald CGO, Unusual Differential Diagnosis of a Swollen Toe, J Rheumatology 2004, 31:3,617-619 (im Cache).
(Datum: 8.3.2005)
Tagungsankündigungen
- Frühjahrstagung des Borreliosebunds Deutschland, 9. und 10. April 2005, Fulda,
- 5. Kasseler Symposium, 29. Oktober 2005,
- Fortbildungstagungen - Neurologie, 27. April 2005, 1. Juni 2005.
(Datum: 28.9.2004)
Gefahr durch Zeckenbisse, ZDFmediathek, 28.9.04.
Es ist ein engagierter und genau recherchierter Beitrag zur Problematik der unzureichenden Diagnose und Arztunkenntnis und mit einem ernsten Hilferuf von Dr. Volker Fingerle (Nationales Referenzzentrum Borrelien (NRZ)), Abteilung Bakteriologie des Max-von-Pettenkofer-Instituts.
(Datum: 11.9.2004)
US National Institutes of Health (NIH) schlägt kostenlosen öffentlichen Zugang zu Forschungsdaten vor.
Das NIH (US-Gesundheitsbehörde) hat eine wesentliche Politik-Änderung vorgeschlagen, die alle Wissenschaftler binden würde, welche Gelder von den NIH erhalten: Sie müßten danach die Resultate ihrer Forschung der Öffentlichkeit kostenlos zur Verfügung stellen.
(Datum: 30.8.2004)
4. Kasseler Borreliose-Symposion
8. September 2004, im B00rgerhaus Obervellmar, Holl03ndische Str. 129, 34246 Vellmar
(Datum: 8.8.2004)
Wie lange muß eine Zecke an unserem Köper sein, um uns zu infizieren?
Art Doherty über Tick-Attachment:
http://www.geocities.com/HotSprings/Oasis/6455/tick-attachment.txt
(Datum: 11.5.2004)
Zeckenbiss und die Folgen, Deutschlandfunk, Journal am Vormittag, Sprechstunde mit Studiogast Prof. Dr. Emil Christian Reisinger, Direktor der Abteilung für Tropenmedizin und Infektionskrankheiten, Klinik für Innere Medizin, Universität Rostock, Moderator: Carsten Schroeder (Mitschnitt zu bestellen gegen Verrechnungsscheck über 10 EUR bei Deutschlandfunk Marketing & Service GmbH, Raderberggürtel 40, D - 50968 Köln.):
- Seine Einführung in die Problematik
- Hörerfragen und seine Antworten
Man beachte, daß die im Mitschnitt angegebene Hörer-Telefonnummer nur für die Dauer der Sendung galt.
Anmerkungen:
- Herr Reisinger machte u.a. folgende Aussagen:
- Resistenz: Borreiien seien bezüglich Antibiotika gut empfindlich. Ihm sei aus der Literatur kein einziger Fall von Borrelien-Antibiotika-Resistenz im mikrobiologischen Sinne [im Gegensatz zu ihrer Widerstandsfähigkeit im Wirtskörper, die er nicht erwähnte, J. Gruber] bekannt.
- Gute Heilungsaussichten: Chronische Borreliose komme vor, aber sei gut heilbar mit Antibiotika, wenn sie adäquat therapiert wird, d.h. mit intravenösen Antibiotika, mit den richtigen Antibiotika, ausreichend lange und kontinuierlich (nicht am Wochenende mit den Infusionen aussetzen).
- Therapiedauer: Auf eine Hörerfrage nach der Thearapiedauer für Borreliose-Stadium III (im Gegensatz zu Stadien I und II, für die er die gängigen 10 - 20 Tage nannte) mochte er nicht antworten (seine Antwort auf diese Frage war sinngemäß: "Es wäre nicht seriös, diese schwierige Entscheidung nur auf telefonische Konsultation zu gründen.") Ich entnehme der Antwort, daß er die Therapiedauer individuell bemißt, d.h. abhängig vom klinischen Bild und dem Verlauf der Therapie.
- Labortests zur Diagnose: Antikörper-Tests [ELISA, Westernblot] haben in Borreliose-Stadien I und II geringe Sensitivität und Spezifität.. Im Stadium III haben sie sehr hohe Sensitivität und Spezifität, d.h. in den meisten Fällen finden sich Antikörper gegen Borrelien-Proteine.
- Prophylaxe: Ihm sei nur eine Studie (nämlich aus dem Jahr 2001) an 500 von einer Zecke gebissenen Menschen) bekannt, in der etwa 250 Menschen einmal 200 mg Doxycyclin direkt nach dem Zeckenbiß gegeben wurde. Die restlichen Gruppenmitglieder hatten nur einen Placebo erhalten. In der mit Doxy behandelten Teilgruppe seien weniger Wanderröten aufgetreten. Dies sei jedoch nur eine Studie, und sie habe nur eine kleine Anzahl von Menschen umfaßt. Weil nur etwa 1 % der Gebissenen eine Borreliose entwickelten, könne er aus dieser Studie nicht ableiten, daß Doxy prophylaktisch gegeben werden solle. Man solle vielmehr abwarten, ob sich Borreliose-Symptome einstellen.
- Herr Reisinger erwähnt nicht die Gasser-Reisinger-Pulstherapie.
- Er versäumt, auf neuere Forschung zum Therapieversagen hinzuweisen, z.B.
Weitere Anmerkungen von Jutta Zacharias.
(Datum: 6.4.2004)
Marie Kroun, Geschichte der Borreliose in Europa
Links in PPT, PDF & DOC Format:
http://lymerick.ulmarweb.dk/Bb-history.ppt
http://lymerick.ulmarweb.dk/Bb-history.pdf
http://lymerick.ulmarweb.dk/Bb-history.doc
das letztere ist eine kürzere 11-Seiten-Version, die beim Ausdrucken der Literaturliste Papier spart. Man kann sie auch hier finden.
"Es geht dabei um die Geschichte der Borreliose in Europa.
Ich finde die Sache sehr interessant, insbesondere deshalb, weil damit klar wird, das es in Europa schon ganz lange Hinweise auf die Borreliose gab bevor der Erreger dann erst in den 70/80er Jahren in den USA von Willy Burgdorfer entdeckt wurde.
Da oftmals auch auf alte deutsche Texte verwiesen wird, ist die Sache bestimmt auch für Leute interessant, die nicht so gut Englisch verstehen." (Peter Rohleder)
(Datum: 28.1.2004)
ILADS, International Lyme and Associated Diseases Society, A Professional Medical and Research Organization, "New Treatment Guidelines For Lyme Disease: World-Wide Standards Are Based On Evidence.
"... Diese Richtlinien werden Ärzten wesentliche Ermunterung und Validierung ebenso wie Zutrauen geben, die ihnen manchmal fehlten, wenn sie die Krankheit zu finden und zu behandeln versuchten.
Fehlinformation und unvereinbare Ansichten haben Inkonsistenzen und Verwirrung hervorgerufen, manchmal verbunden mit einem hohen Preis für die Patienten.
Die ILADS-Richtlinien stammen von einigen der am meisten angesehenen, in Publikationen vertretenen und erfahrenen Experten auf dem Arbeitsgebiet. Diese Richtlinien sollten einen großen und positiven Einfluß im Leben der Patienten haben.
In ILADS sind mehr als 200 medzinische Experten zusammengefaßt, die sich auf die direkte Behandlung von Lyme-Patienten spezialisiert haben. Die ILADS-Mitglieder, welche die Richtlinien verfaß haben, sind Krankenhaus-Ärzte, Wissenschaftler, Angestellte von kommunalen Gesundheitsdiensten und Patienten-Anwälte."
(Steven Phillips, Präsident, ILADS)
For more information and a copy of the guidelines, go to
- ILADS' website or
- print out order form and -including payment- mail it to
ILADS
PO Box 341 461
Bethesda, MD 20827-1461, USA
Phone: +1 301 263 1080
Fax: +1 301 263 0776
email: lymedocs@aol.com.
(Datum: 27.1.2004)
Carroll JF, Kramer M, Winter activity of Ixodes scapularis (Acari: Ixodidae) and the operation of deer-targeted tick control devices in Maryland, J Med Entomol. 2003 Mar; 40(2): 238-44..
Host-seeking activity of adult blacklegged ticks, Ixodes scapularis Say was monitored by flagging during winter months in Beltsville, MD. Ticks were active many days during January and February, the coldest months, with some captures made when there was 70% snow cover and temperatures as low as -2 degrees C
(Datum: 22.1.2004)
Pal U, Yang X, Chen M, Bockenstedt LK, Anderson JF, Flavell RA, Norgard MV, Fikrig E., "OspC facilitates Borrelia burgdorferi invasion of Ixodes scapularis salivary glands." J Clin Invest. 2004 Jan; 113(2): 220-30. (Abstract)
(Datum: 28.8.2003)
LYME DISEASE ASSOCIATION (LDA) ANNOUNCEMENT
Burrascano/Bransfield DVD available
September 1, 2003 - The LDA will begin accepting orders for a new DVD featuring Joseph Burrascano, MD (internist) from East Hampton, New York, and Robert Bransfield, MD (psychiatrist) from Red Bank, New Jersey, discussing various aspects of Lyme disease.
No other formats are available. Allow 6-8 weeks for delivery.
Please send your name & address and a $15 check or money order payable to:
Lyme Disease Association, Inc.
PO Box 1438
Jackson, NJ 08527
USA
Pat Smith,
President,
Lyme Disease Association
PO Box 1438
Jackson, NJ 08527
Tel.: +1 888 366-6611,
FAX: +1 732 938-7215
(Datum: 5.5.2003)
Grüße von J.J. Burrascano
(Datum: 28.4.2003)
3. Kasseler Borreliose-Symposium, Vellmar, 18.6.2003
(Datum: 5.8.2002)
Borreliose.org
ist die inhaltlich sehr farbige, neue Borreliose-Website von Jutta Zacharias
mit einer sorgfältigen Auswahl von medizinischer Fachliteratur.
(Datum:
23. 1.2003, 18.8. 2004, 29.9.2004)
Ellen
Lubarsky Things that need to be done to help LLMD's in New York State,
z.B. kann man
-
die Lobby-Gruppe FAIM
(Foundation for the Advancement of Innovative Medicine - Stiftung zur Förderung von innovativer Medizin-) unterstützen,
"This group has so many physicians who think outside the box that I
encourage you all to join FAIM, the Foundation for the Advancement of
Innovative Medicine.
The New York State group of Lyme patients has worked with FAIM since 2000 when Dr.Burrascano
joined and encouraged us to work with the lobbyist from FAIM.
Since that time Monica Miller, the lobbyist, has done an unbelievable
job for us. I don't know what would have happened to our Lyme doctors
if we had not had the leadership of Monica.
So please help keep FAIM functioning forever. There are plenty of
other issues on which our interests will coincide with those of FAIM.
To read about the organization please go to www.faim.org. To join, go
to www.faim.org/benefits.htm. You can access a form to fill out and mail in."
Ellen Lubarsky
-
zu Legal Defense Funds beitragen (Ken Liegner Legal Defense Fund).
- NEU
Datum: 29.9.2004
The OPMC bill is in some trouble. The New York State Department of
Health is putting a great deal of pressure on the Governor to veto the
bill.
While the Department of Health has significant power, don't forget that
we as voters also have a great deal of power IF we make our voices heard
in sufficient numbers.
Since Governor Pataki would like to be President some day, he will be
responsive to requests from voters throughout the country.
If you have not written and called Governor Pataki in the past two
weeks, please do so .
- Click here to email Governor Pataki:
http://161.11.3.75/
scroll to the middle of the page to send Governor
Pataki an email.
Write the message...
"Please sign Bill A4274b for OPMC Reform."
- Call Governor Pataki's office:
518-474-8390
Say... "Please sign the bill for OPMC Reform , A4274b"
- Please again be creative in getting friends, family and community
organizations to do the same.
- Please email me (ellenlu@webtv.net) if you are able to volunteer
some time to make calls and faxes. We will be arraanging for people to
call and fax information about the law to physicians in NYS, encouraging
them to contact Pataki.
- For information on what this bill is and why we all urgently need it
to protect our medical care, please see:
http://flash.lymenet.org/ubb/Forum1/HTML/026443.html
Thanks,
Ellen
Lyme Diagnose im Staat New York - Das New York State Department of Health hat in einem "Alert" Anfang April 2002 mitgeteilt,
-
daß eine Diagnose auf Lyme allein vom klinischen Erscheinungsbild des Erkrankten her getroffen werden kann.
-
Serologische Tests können bei Patienten mit Spätsymptomen (later stage symptoms) als unterstützende Information für die Diagnose herangezogen werden.
Die neue Haltung, die damit auch das Office of Professsional Medical Conduct (OPMC) vertritt, steht wahrscheinlich im Zusammenhang mit dem Hearing in Albany. Viele Hunderte von Aktivisten haben sich trotz ihrer Krankheit -besonders im vergangenen Jahr- bei dieser basisdemokratischen Arbeit sehr eingesetzt (Info z.B. bei FAIM und LymeInfo.net). Wir empfinden Dankbarkeit gegenüber Antonia C. Novello, die -in ihrer Eigenschaft als NYS Health Commissioner- diesen bedeutsamen Positionswechsel ausgeführt hat. Nachricht von Monica Miller: Am 16 April 2002 hat die New York State Assembly der Abstimmung des Health Committee zugestimmt - mit über 75 Zustimmungen von beiden Seiten der Kontroverse - eine bemerkenswerte Tat dieses gewöhnlich in Fraktionen aufgeteilten Gesetzgebungskörpers.Der Chairman Gottfried (D) und Abgeordneter Joel Miller (R) argumentierten mit den zunächst ablehnenden Abgeordneten und gewannen alle Stimmen bis auf eine - die von Pete Grannis (D, Chairman des Versicherungs-Kommittees). Wortlaut
der NYS Assembly Resolution K02155.
Die NYS Assembly kann eine Resolution allein beschließen.
Nach den am 17. Oktober 2002 und 21. Juli 2004 erfolgten einstimmigen Zustimmungen des Senats (S. 969) und der New York State Assembly wird die OPMC Reform Bill nun George Pataki, dem Gouverneur von New York, zur Unterschrift vorgelegt. Er macht sie mit dieser Unterschrift zum Gesetz.(siehe auch www.lymesociety.com). OPMC Reform Bill im Staat New York
(Chronologie der Ereignisse, Hintergrund, Text der Reform-Bill, Why do we need an OPMC-Reform-Bill) Ellen Lubarsky:
" Kurz zusammengefaßt ist dieser Bill zweimal vom [New York State] Assembly zugestimmt worden, sie ist aber [noch] nicht aus den Kommittees des Senats herausgekommen. Diese Bill würde die OPMC neugestalten in der Weise, daß sie den Ärzten angemessene Mittel zum eigenen Schutz vor ungerechtfertigter Verfolgung gewähren würde.(Stand: 2.10.03)
Im Einzelnen:
Am 18. Juni 2002 ist die OPMC Reform
Bill A11330B einstimmig beim Assembly Codes Committee durchgegangen und
am 20. Juni durch die New York State Assembly einstimmig beschlossen worden.
...
Am 24 Mai 2002 wurde die OPMC Reform Bill als S.7466 durch William Larkin (R, Lower Hudson Valley Region) in den New York Senate ingebracht.
... Die New York State Assembly hat Anfang Mai 2004 die Bill A7365a verabschiedet. Das ist die Bill, welche die OPMC daran hindert, Ärzte in New York nur wegen ihrer Art der Borreliose-Behandlung zum Ziel ihrer Untersuchung zu machen.
... Senator Leibell, der ein guter Freund der Lyme-Community ist, wird diese Bill im New York State Senate befürworten.
...
Etwa vor einem Jahr (also im Jahre 2002) haben wir uns
für die Medically Necessary Care Bill
eingesetzt, die noch nicht gilt. Wenn gültig, wird sie wird festlegen,
daß durch Gesetz bestimmt wird, was medizinisch notwendig ist. Bisher
kann im Staat New York eine Krankenversicherung das allein bestimmen."
FREQUENTLY ASKED QUESTIONS ABOUT WHAT'S UP WITH THE OPMC REFORM BILL
August 18, 2004
Q. I THOUGHT THE OPMC REFORM BILL HAD TEN DAYS TO BE SIGNED OR VETOED BY THE GOVERNOR.
A. That is ten days after it is sent to him . It has not yet been sent.
Q. WHO DECIDES WHEN IT IS SENT TO THE GOVERNOR? A. Assembly Health Committee Chairman, Richard Gottfried, makes that decision.
Q. WHEN WILL THE BILL BE SENT?
A. The absolute deadline for sending the bill to the Governor is some time in December. Obviously , we would want the bill sent to him before that to avoid wear and tear on our nerves.
The bill will be sent up to the Governor when Assemblyman Gottfried thinks it is likely that it won't be vetoed. Currenty some behind the scenes work is helping to clairfy that.
It is our job, by generating calls and emails to Pataki, to create a climate in which it is likely that the Governor will sign the bill.
Q. WHAT HAPPENS IF GOVERNOR PATAKI DOES NOT EITHER SIGN OR VETO THE BILL AFTER IT IS SENT TO HIM?
A. If Pataki does not sign or veto the bill within the10 day limit after he receives it, the bill automatically passes.
Q. SINCE THE LEGISLATURE PASSED THE BILL UNANIMOUSLY, WHY DO WE HAVE TO WORRY ABOUT WHETHER THE GOVERNOR WILL SIGN IT?
A. The Governor has vetoed MANY bills that have been sent to him by the legislature, even those that passed unanimously and those that he helped pass the legislature. In our case, we do not know how the Governor will vote. We know that when we started protesting the OPMC persecution of our LLMDs, the Govenor sent all of our letters to the Commissioner of Health without reading them. (The OPMC is part of the Deparment of Health).
It's four years later, and we have a lot more political clout than we had then. But we don't know what effect any possibe opposition from his Commissioner of Health will have on him.
Another pitfall could be insurance company opposition to the bill. There are probaby many more political influences at work on Governor Pataki that we are not even aware of .. So we have to use ALL our strength to urge him to sign the bill He has to be made aware that there is a strong public demand for this bill - stronger than any interests that might be opposing it.
Q. WHAT HAPPENS IF THE GOVERNOR VETOES THE BILL?
A. Oy! Bite your tongue. You don't want to know from it.
We would then try to get the legislature to override the Governor's veto.
I don't know what the chances are that they will do that. But I do know that trying to get them to override the veto would be some of the hardest work we have ever had to do.
It would involve getting Republican legislators to override the Republican Governor's veto, which could mean being ostracized by their party.
So, please , let's make it easy on ourselves and pressure the Governor to sign the bill now.
Q. WHAT HAPPENS IF THE BILL IS VETOED AND THE LEGISLATURE DOES NOT OVERRIDE THE VETO?
A. You keep asking those uncomfortable questons. This one you really don't want to know from.
We would need to start from scratch, from where we were in 2002. The bill would have to be reintroduced in both houses of the legislature - and likely have to repeat all the struggle that we have been through since then.
In the meantime, it would be very likely that the OPMC would try, and possibly succeed, in taking the medical licenses away from more of the LLMD's in NYS, This would almost definitely mean losing more LLMDs across the country.
More reason to get everybody you know to contact the Governor now.
Q. WHAT CAN WE DO NOW TO CONVINCE THE GOVERNOR TO SIGN THE OPMC REFORM BILL?
A. I'm so glad you asked.
1. Click here to email Governor Pataki. Scroll to the middle of the page to send Governor Pataki an email. Write the message... Please pass Bill #A4274b, for OPMC Reform.
2. Call Governor Pataki's office: 518-474-8390 Say... "Please pass the bill for OPMC Reform."
3. Call Senator Kemp Hannon's office: 518-455-2200 (address: Hon. Kemp Hannon, Chairman Senate Health Committee, Room 609 LOB
Albany, NY 12247, USA). Thank Senator Hannon for sponsoring the OPMC Reform Bill. Ask him to please encourage Governor Pataki to sign the OPMC Reform bill.
4. Contact all your friends and family, no matter where they live and whether or not they have Lyme, and ask them to do steps 1-3 above.
5. Go to the Headlines page of Lymenet www.lymenet.org Click on the link for the OPMC Flyer. Print it out and distribute it. Make sure your LLMD has a copy to give to his/her patients.
6. Join the Foundation for the Advancement of Innovative Medicine, FAIM. This organization has paid the lobbyist who has worked with us for our years. Go to www.faim.org/benefits.htm Print out the application and mail it in with your dues.
Q. IS EVERYONE SUPPOSED TO DO THE ABOVE, NO MATTER WHERE THEY LIVE AND WHETHER OR NOT THEY HAVE LYME?
A. Yes!
Q. WHAT IS THE OPMC REFORM BILL AND WHY DO WE NEED IT?
A. It's a long story, which you can find at http://flash.lymenet.org/ubb/Forum1/HTML/026443.html
Q. WHAT WILL WE DO IF THE GOVERNOR SIGNS THE BILL?
A. We will have the biggest party in the history of Lymeland.
Thank you,
Ellen
Mehr von
(Datum: 8.10.2002)
Burrascano Legal Defense Fund (B. Rechtshilfefond) ist geschlossen.
Über Lymenet.de wurde 655 US$ + 30 US$ beigetragen. Monica Miller hatte einen BLDF ins Leben gerufen und dankt nun allen, die sich beteiligt haben ("Give my best regards to all the donors. MM")
Wir danken auf diesem Weg allen Mitgliedern der Borreliose-Selbsthilfegruppen in Berlin-Brandenburg und Kassel und den Teilnehmern der Jahreshauptversammlung des Lyme-Borreliose-Bunds in Fulda sehr für ihre Beteiligung. Große Beiträge haben wir auch von Einzelpersonen bekommen, und ihnen möchten wir hiermit herzlich danken. Insgesamt haben sich etwa 200 Personen beteiligt.
J.J. Burrascano am 14.3.2002: "Ich muß unmittelbar jetzt weitere $ 7500 auftreiben für Rechnungen, die überfällig sind, und da sind viele weitere, bei denen ich im Verzug bin."
Falls Sie zum Rechtshilfefond beitragen möchten, haben Sie die Wahl zwischen folgenden Wegen:
- Wenn Sie ein Konto bei einer Bank in den USA haben,
können Sie einen Scheck ausstellen auf FFOLLMD und an die folgende Adresse schicken:
FFOLLMD
c/o Long Island Lyme Association
P O Box 1842
North Massapequa, NY 11758
USA
-
Sie können einen Scheck von jeder -auch einer nicht-amerikanischen- Bank ausstellen auf "Dr. Burrascano Legal Defense Fund" und schicken an
Burrascano Legal Defense Fund
c/o Monica Miller
PO Box 410
Kinderhook, NY 12106
- Sie können die Spende überweisen auf mein Konto:
Kontoinhaber: Dr. Joachim Gruber
Konto-Nummer: 416 8530
Bank: Deutsche Bank, Hamburg
Bankleitzahl: 200 700 24
Verwendungszweck: Burrascano Legal Defense Fund
Ich werde die Beiträge weiterhin sammeln und regelmäßig in die USA überweisen.
Mit Mastercard oder Visa kann man in dieser Sache leider nicht arbeiten.
(Datum: 15.5.2002)
Umfrage
zur Borreliose-Behandlung
mit Moderner
Chinesischer Medizin.
(Datum: 21.12.2001)
Bericht
über die Informationsveranstaltung des Borreliose Selbsthilfe e.V.
Berlin-Brandenburg am 17. Oktober 2001 im St. Marien-Krankenhaus in Berlin-Lankwitz
-
Prof. Dr. med. R. von Baehr:
Der Lymphozytentransformationstest
für Borrelien: Neue diagnostische Möglichkeiten für Problemfälle
-
Prof. Dr. med. Kursawe:
Klinik und Therapie der Neuroborreliose
unter Einschluß der Pulstherapie
(Datum: 23.10.2001, 5.11.2001, 18.1.,
1.2., 10.2.2002, 20.2.2002)
Am 27.11.2001
veranstaltete der New York State Gesetzgeber in Albany, der Hauptstadt
des Staates New York, ein öffentliches Hearing zur Lyme-Kontroverse
(New York State Assembly resolution).
Zusätzlich gab es am 31.1.2002
in New York City, im Assembly Hearing Room, 19th floor, 250 Broadway um
10:00 Uhr ein Hearing über die Vorgehensweisen
des OPMC (Office for Professional Medical Conduct). FAIM
hält eine Mitschrift
dieses Hearings bereit, ebenso LymeInfo.Net.
Vorläufige Info zum Hearing
am 31.1.02: "The testimony lasted for a little over 3 hrs. and the final
words were (instructing the OPMC)... "Leave the drs. alone that treat lyme
disease and leave the controversy up to the scientists! They will over
time figure out what lyme disease is and is not."
Siehe auch Lyme
disease more prevalent and misunderstood than previously thought.,
Excerpts from Public Law 107-116 Signed by President Bush 1/10/02.
(Datum: 4.8.2001)
Willy
Burgdorfer (siehe auch hier)
in Volume 1, 2001 von Lymelight, einer Publikation der Lyme
Disease Foundation:
"Wir wissen, daß Lyme Borreliose
Antibiotika widerstehen kann. Also, zu sagen, jemand sei geheilt, weil
sie eine bestimmte Menge von Antibiotika erhalten haben, ist Unsinn ..."
"Es gibt keine Lyme-Borreliose-Experten",
sagt er. "Zu viel muß noch gelernt werden über die Physiologie
und Biologie des Organismus, und wie er im menschlichen Körper wirkt."
|
|
{kind=link}